
Tourniquet Use
Warning
Objectives
To outline best practice in the use, reassessment, replacement and conversion of tourniquets for the management of massive external haemorrhage.
Scope
This emergency procedure guideline describes best practice regarding the application, replacement and conversion of tourniquets for controlling massive external limb haemorrhage.
Guidance is provided in the use of both issued tourniquets and the use of improvised tourniquets during extreme circumstances.
There are separate guidelines covering the management of massive junctional haemorrhage including wound packing and the use of haemostatic dressings.
Massive haemorrhage is bleeding that is so severe the casualty will die within minutes if it is not controlled. It is the leading cause of preventable death on the battlefield.
Massive haemorrhage has previously also been described as ‘catastrophic haemorrhage’. The current terminology aligns with that used by the Tactical Combat Casualty Care (TCCC) trauma system.
Audience
This guideline is for the use of registered healthcare professionals in forward medical locations or in an Emergency Department on deployed operations.
Initial Assessment & Management
Indications for Tourniquet Use
- Traumatic amputation of a limb
- Massive haemorrhage from a limb, from a site that allows a tourniquet to be used
- Haemorrhage from a limb that cannot be controlled despite optimal application of pressure and haemostatic dressings
Preparation
Check that the tourniquet is undamaged and is in a serviceable condition.
Exposure to the environment may degrade a tourniquet’s function. Tourniquets should be regularly and carefully checked following prolonged exposure to extreme conditions that may include heat, sand, freezing temperatures, abrasion. These factors may reduce a tourniquet’s reliability and functionality - increasing the risk of tourniquet failure when used.
Procedure
Position - Place the tourniquet 5–7 cm (approx 2-3 fingers' breadth) above the bleeding site. If the site isn’t visible, ensure that the position is clearly proximal to the injury. Do not place directly over a joint.
Apply - in non-permissive environments (care under fire), apply over clothing. In semi-permissive/permissive environments, rapidly expose the limb and apply the tourniquet directly to skin.
Tighten the band - pull the tourniquet band tightly around the limb to remove all slack.
Secure the device - use the tourniquet mechanism (clip, buckle or fastner) to hold the device and tightening system securely in place.
Tighten Until Bleeding Stops - use the tourniquet’s tightening mechanism (windlass, ratchet, dial) until distal bleeding has clearly stopped.
Secure and Record - lock and secure all components as per tourniquet’s design. Record the time of application clearly on the casualty and on any casualty documentation.
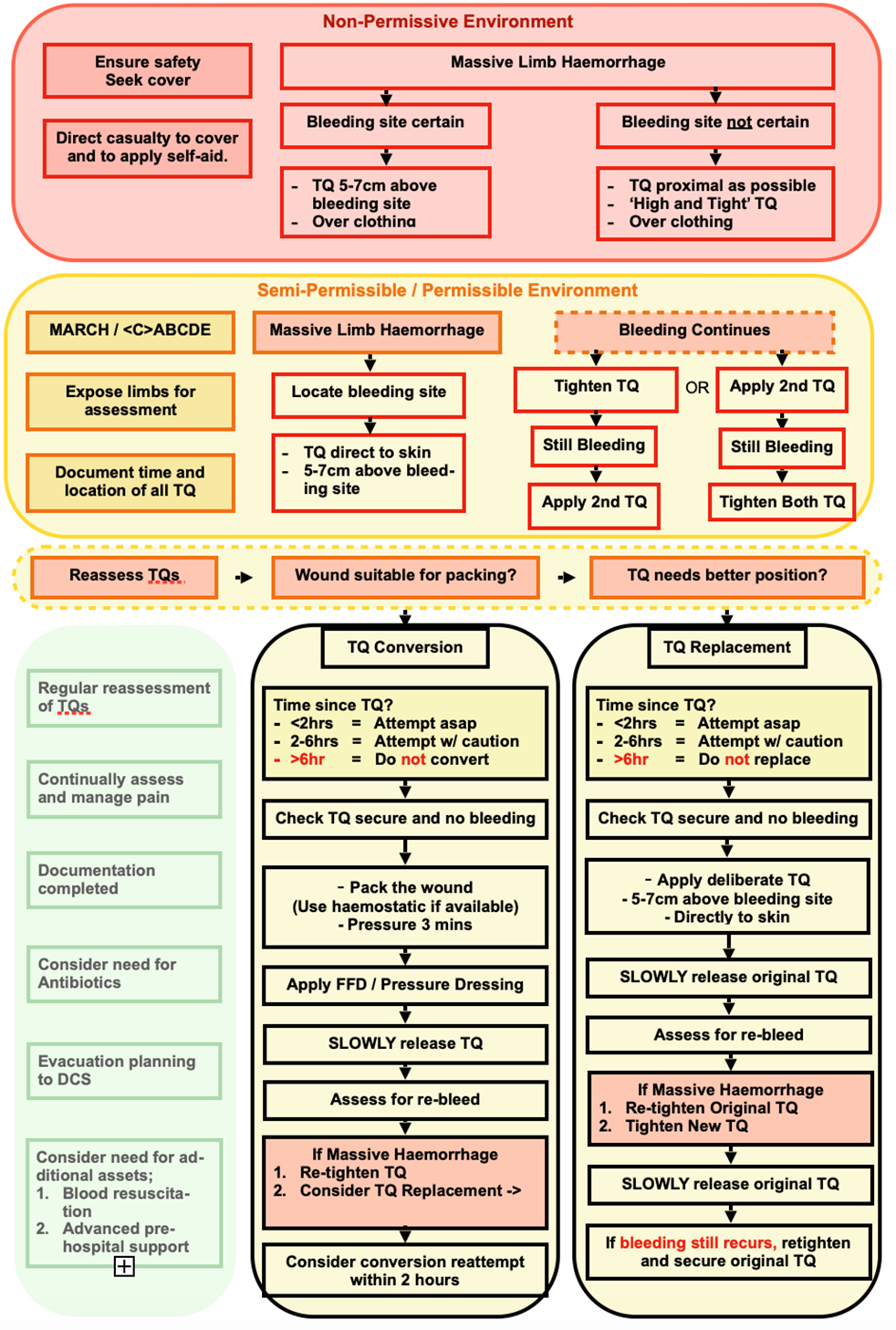
Considerations in a Non-Permissive Environment
The safety of the casualty and the medical provider is paramount. The casualty should be directed to move to cover and self-apply a tourniquet if possible, while contact is ongoing.
If the bleeding site is obvious, and the tactical situation permits, the tourniquet can be applied over the casualty’s clothing, 5-7cm clearly above the bleeding site.
If the bleeding site is uncertain, or the tactical situation does not permit (darkness, highly confined), apply the tourniquet as proximal as possible on the bleeding limb. This can be applied over the casualty’s clothing.
The proximal application of a tourniquet over clothing in a non-permissive environment may be referred to as ‘High and Tight’ application. The term ‘Hasty tourniquet’ may also be used. This method of application carries a high risk of adverse consequences and should be considered a Care Under Fire intervention only. A tourniquet applied by this method must be assessed and re-positioned if possible, at the earliest safe opportunity.
If massive haemorrhage persists despite the application of the tourniquet, apply a second tourniquet proximal and adjacent to the first.
Record the time of tourniquet application clearly and mark “T” and the time on the casualty’s forehead using a permanent marker. Alternatively, mark the date and time on the affected limb or the chest. Aim to record an ATMIST card if/when possible.
Considerations in Semi-Permissive/Permissive Environments
Use a systematic approach (MARCH) to assess the injured casualty.
Expose all limbs to thoroughly assess for uncontrolled massive haemorrhage. If massive haemorrhage to a limb is identified then locate the source of bleeding.
Do not delay tourniquet application, but if possible direct the casualty or a buddy/helper to elevate the bleeding limb and apply direct pressure to the wound while preparing to apply a tourniquet.
Apply the tourniquet directly to the skin (not over clothing), 5-7cm above the bleeding site. Follow the procedure to secure and tighten the tourniquet until bleeding is controlled.
If bleeding continues;
- Consider tightening the original tourniquet’s windlass further and re-assess.
and / or
- Apply a second tourniquet immediately proximal to (above) the first tourniquet and re-assess.
If bleeding still continues, re-assess to ensure no other bleeding sites have been missed. Use wound packing with haemostatic dressings and direct pressure to attempt to gain control.
Record the time of tourniquet application clearly and indelibly on the device or, if necessary, on the patient's cheek or forehead (with a 'T'), and document on the casualty record card. Recording the time of tourniquet application, and ensuring this information travels with the casualty, is critical for the re-assessment and consideration of replacement and conversion of tourniquets.
Improvised Tourniquets
Improvised tourniquets are only to be used in extremis where an issued tourniquet is not available.
Expose the wound and identify the source of bleeding. Apply, or direct others to apply, direct pressure while preparing items.
Suitable items:
- Band material: Flexible cloth at least 100 cm long and 5 cm wide (e.g. folded triangular bandage, strip of uniform, necktie).
- Windlass: Rigid rod 0.5–2.5 cm in diameter, 10–15 cm long (e.g. entrenching handle, weapon cleaning rod, thick branch).
Avoid using narrow materials (<5cm wide) such as cords, wires, zip ties, shoelaces or narrow belts; ensure that anything used as an improvised windlass is not fragile or slippery.
Place the band 5–7 cm (approx 2-3 fingers' breadth) above the bleeding site. If the site isn’t visible, ensure that the position is clearly proximal to the injury. Do not place directly over a joint.
Pass the band material around the limb and loop the free ends to form the first half of a reef/square knot. Place the windlass over the half-knot and repeat the loop of the free ends to complete the knot.
Twist the windlass in one direction until bleeding stops, then secure in place by tying the free ends of the knot tightly around the windlass. If available, use tape or another dressing to further stabilise/secure.
Mark and record the time of application.
Close monitoring of an improvised tourniquet is especially important as there is a higher risk of displacement. Any improvised tourniquet should be replaced with an issued device as soon as practicable.
Tourniquet ReassessmentRegular reassessment of tourniquets is essential:
Is it still working? Tourniquets must be closely monitored and regularly reassessed to ensure they are effectively controlling any massive haemorrhage. This will require exposure of the limb and assessment of the bleeding site.
Can it be converted? As a situation changes and/or a patient is transferred, the environment is likely to become more permissive and additional resources will become available, allowing a wound to be controlled without a tourniquet using other techniques such as wound packing, pressure dressings and haemostatic dressings.Reassessment is especially important:
- After any patient movement or transfer to ensure tourniquets have not been dislodged.
- When treatment such as fluids (including blood components) have been administered that may have restored the patient's blood pressure.
In addition, all tourniquets should be promptly and carefully reassessed on any handover of care including arrival at a medical treatment facility.
Remember that a "High and Tight" or "Hasty Tourniquet" must be either replaced with a tourniquet sited close to the wound or converted using alternative methods of haemorrhage control as soon as it is safe to do so. Convert if possible; replace if not.
Tourniquet Replacement
Tourniquet Replacement is used:
- When a "High and Tight" or "Hasty Tourniquet" has been used and it is now safe to adjust.
- When an ordinary tourniquet has been sited more than 5-7cm above the bleeding site.
- When clothing has been trapped under a tourniquet and repositioning may be possible.
- When tourniquet conversion has failed.
The aim is to ensure that the tourniquet is optimally placed, directly onto skin, 5-7cm above the bleeding site.
Tourniquet replacement should be undertaken as soon as it is safe to attempt, ideally within 2 hours. Always consider first whether tourniquet conversion may be possible.
Tourniquet replacement can be performed up to 6 hours after original application, but if >2 hours then there is a risk of reperfusion injury - monitoring is recommended, and guidance on management may be found in the CGO on reperfusion injury (link to follow).
Tourniquet replacement should not be attempted forward of deployed hospital care if more than 6 hours have elapsed since tourniquet application: if a tourniquet has been in place for 6 hours or more, the patient requires surgical review and may require limb amputation.
Expose the injury and assess the bleeding site. Consider whether it may be possible to attempt tourniquet conversion - only replace if you cannot convert.
Apply a new tourniquet directly to the skin, 5-7cm proximal to the bleeding site, then attempt to gently release the original tourniquet(s) by slowly unwinding the windlass. Do not rapidly loosen or cut the original tourniquets.
Assess the bleeding site for significant bleeding.
If significant bleeding recurs:
- immediately re-tighten the initial tourniquet
- optimise the position and further tighten the newly applied tourniquet
- again attempt to gently release the original tourniquet
If still unsuccessful, consider applying a second new tourniquet alongside the first.
If all attempts to establish a new tourniquet fail then it may be necessary simply to re-tighten the original tourniquet and leave in place. However, if at all possible a "high and tight" tourniquet should be replaced even if the new tourniquets end up >5-7 cm proximal to the wound this at least preserves as much tissue as possible and reduces the risk of massive reperfusion injury.
Once complete, record and document the time of the new tourniquet placement. Ensure that the duration of initial tourniquet application is also clearly documented so there is an accurate record of total tourniquet time.
Tourniquet Conversion
Tourniquet Conversion is the process of safely replacing a tourniquet with other means of haemorrhage control (usually including a haemostatic dressing and pressure bandage) once bleeding is controlled and the tactical and clinical situation allows. It is done to minimise ischaemic injury to the limb.
Tourniquets applied during care under fire or in other high pressure situations, even by experienced medical personnel, may not be essential for haemorrhage control once the situation is more permissive. This does not mean that the decision to apply a tourniquet was incorrect, but all tourniquets should be carefully reviewed as soon as it is safe to do so, to determine if other measures can control the haemorrhage.
Tourniquet conversion should be undertaken as soon as it is safe to attempt, ideally within 2 hours.
Tourniquet conversion can be performed up to 6 hours after original application, but if >2 hours then there is a risk of reperfusion injury - monitoring is recommended, and guidance on management may be found in the CGO on reperfusion injury (link to follow).
Tourniquet replacement should not be attempted forward of deployed hospital care if more than 6 hours have elapsed since tourniquet application: if a tourniquet has been in place for 6 hours or more, the patient requires surgical review and may require limb amputation.
Expose and assess the wound.
Pack the wound with haemostatic gauze (if available) and maintain direct firm pressure for at least 1 minute, then apply a pressure dressing over the wound to ensure that sustained pressure is maintained. Use ordinary dressings/gauze if haemostatic gauze if not available. Consult the CGO on wound dressing (link to follow) if needed.
Release the tourniquet by slowly unwinding the windlass.
Monitor closely for signs of re-bleeding.
Bleeding may take some time to become evident through the packing and pressure dressing. Close observation of the casualty and bleeding site is essential.
If bleeding restarts:
- If the original tourniquet was optimally sited, immediately retighten
OR
- If the original tourniquet was sited over clothing and/or more than 5-7cm above the wound then replace with a new, optimally site tourniquet.
If the conversion attempt is unsuccessful, consider further attempts after 1-2 hours, unless or until 6 hours have elapsed after original tourniquet application.
Document the time of tourniquet removal, any re-bleeding or complications.
Advanced Assessment & Management
Pneumatic Tourniquets
Tourniquet replacement to a pneumatic tourniquet should be considered as early as possible in a medical treatment facility with damage-control surgery capability.
Always follow device-specific instructions; the approach is similar to that used for replacement with a conventional tourniquet device, as described above. In addition, consider the following:
Cuff width should approximately be more than 1/2 the limb diameter.
Padding should be used under the cuff.
Lowest effective inflation pressure to control distal bleeding should be used. As a guide, for the upper limb aim for 50-100mmHg above systolic blood pressure; for the lower limb, aim for 70-130mmHg above.
Limb Occlusion Pressure (LOP) should be found if time permits, by slowly reducing the pressure to the lowest possible that controls bleeding. Note that LOP is likely to increase during resuscitation as systolic blood pressure rises.
Siting the device requires surgical input to ensure that sites for proximal vascular control are not obscured.
Ensure all personnel are aware that a pneumatic device is in place including anaesthetic and surgical teams.
Document time applied, site, cuff size and inflation pressures.
Prolonged Casualty Care
Casualties who have injuries that require a tourniquet should be evacuated as a high priority (T1). If this is not possible then continue to reassess all applied tourniquets regularly during prolonged casualty care.
Conversion of the tourniquet must be attempted if possible within 6 hours of application. If conversion is not possible or fails then consider replacement of the tourniquet to preserve as much tissue as possible.
Tourniquets are likely to be extremely painful - provide adequate analgesia (link to follow).
The development of compartment syndrome will heighten the urgency of evacuation: monitor the limb for distal sensation, distal motor function and disproportionate pain; see CGO on Compartment Syndrome for further detail (link to follow).
Ensure appropriate antimicrobial cover as per the relevant guidance (link to follow).
Remember to consider early tourniquet conversion (or tourniquet replacement if conversion is not possible) to preserve tissue and reduce reperfusion injury.
Paediatric Considerations
Issued tourniquets are generally effective for most paediatric casualties, and the indications for and principles for applying a tourniquet are the same in paediatric patients. Remember:
- Control of massive haemorrhage remains the absolute clinical priority.
- Reassessment with consideration of tourniquet conversion, or replacement if conversion is not possible, remains essential.
Issued tourniquets may not be effective for casualties with very small limbs, typically those under 2 years of age. Although it may be possible to use an improvised tourniquet, these are often also not effective in very small children, so the best approach is to use direct pressure with haemostatic dressings and pressure bandages.