The app and website was publicly released on 2 Apr 2024
Update Jan 2025
The content continues to undergo review by all our cadres.
The content remains subject to the following provisos: - The content will be subject to continuous update and review - Old content (from previous CGOs) will be converted into the new format, using the new tools and layouts - Content may be moved around - The layout will change and reflect the needs of the user - Content will be created - Content may be deleted/retired
CGO development will continue.
Saf [Updated 21 Jan 2025]
Choking
!Warning
Objectives
To guide the management of choking patients presenting with suspected or confirmed foreign body airway obstruction (FBAO).
Scope
This guideline describes the recognition, initial management and subsequent resuscitation, if required, of choking patients due to foreign body airway obstruction.
It does not cover the management of airway obstruction due to other medical causes (such as anaphylaxis, severe acute angioedema) or due to maxillofacial trauma. For management of these presentations see separate CGO guidance.
Audience
This guideline is intended for the use of registered healthcare professionals fulfilling a general role in a forward medical location or in an Emergency Department on deployed operations.
Initial Assessment & Management
Recognition
Foreign body airway obstruction should be suspected in any casualty with sudden respiratory distress and/or inability to speak or cough, especially if distress is following eating, or following play/handling small objects in children.
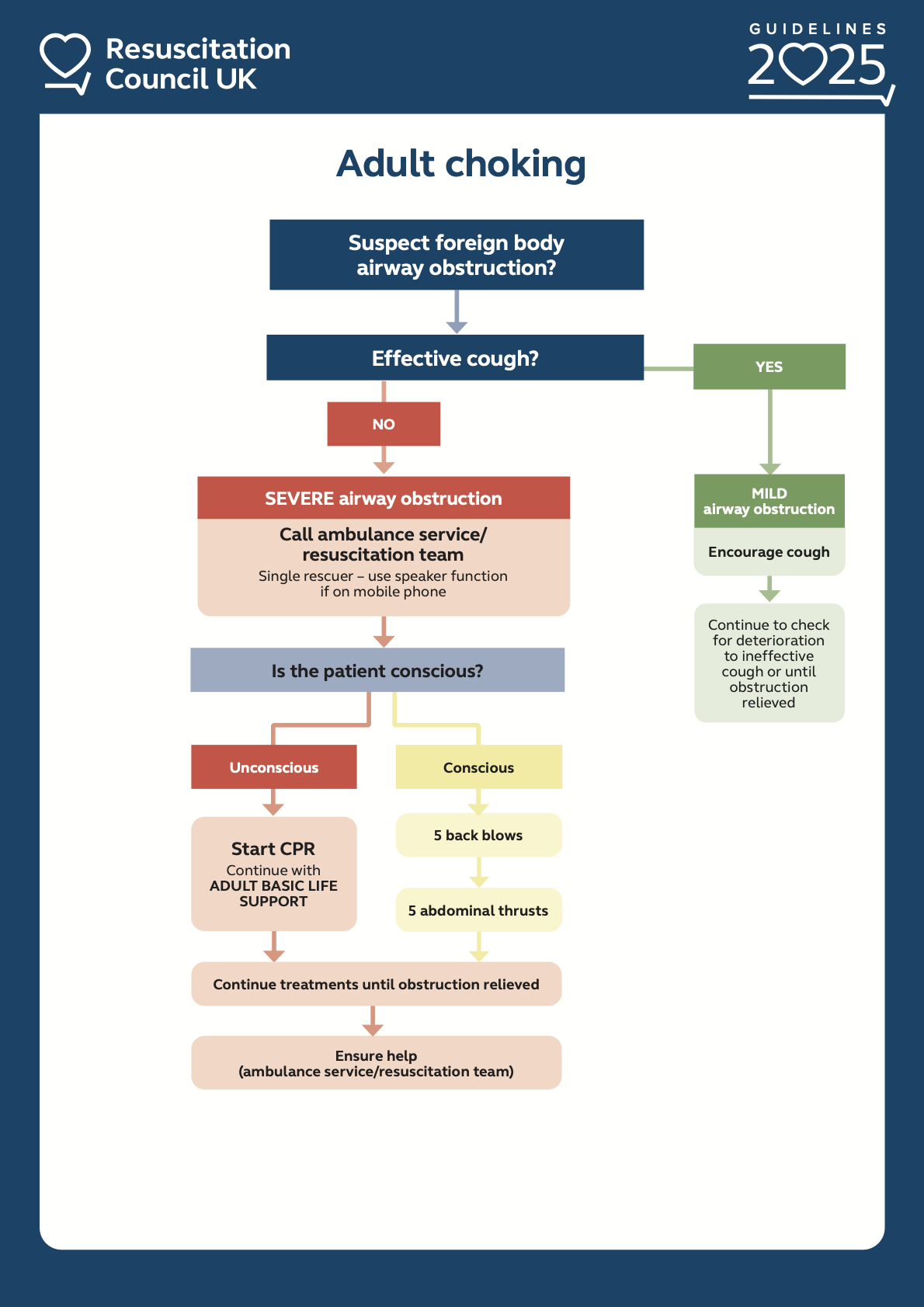
Differentiate severity of airway obstruction based on cough effectiveness:
Effective cough = Mild airway obstruction.
Casualty may be able to speak.
Cough is strong and effective.
There is evident airflow via nose and/or mouth.
Often noisy breathing may be present.
Ineffective cough = Severe airway obstruction. This is a time-critical emergency.
Inability to speak or cough.
Cough is weak.
Silent or minimal airflow.
Clutching or pointing towards their throat.
Cyanosis or rapidly reducing consciousness.
If able, ask the casualty ‘Are you choking?’ in order to confirm the diagnosis. Do not allow this to delay Immediate Actions.
Immediate Actions
Management of Mild Airway Obstruction
Encourage the casualty to continue coughing.
Optimise their position. If able - stand casualty up with support and have them bend slightly forward. This will aid them clearing the obstruction if dislodged by the cough.
Avoid back blows or abdominal thrusts at this stage.
Keep encouraging coughing for as long as they are able to maintain an effective cough.
Continually re-assess and reassure the casualty.
Prepare for rapid deterioration and/or the patient tiring.
Management of Severe Airway Obstruction
Immediately call for expert / additional help. This is a time-critical emergency.
Do not delay initiating immediate management, additional help should be requested concurrently where possible.
Conscious Casualty with Severe Airway Obstruction
Back Blows
Deliver up to 5 back blows. These are forceful strikes between the casualty’s shoulder blades using the heel of the hand.
Check whether the airway obstruction has cleared after each blow.
If 5 back blows have not relieved the obstruction, proceed to abdominal thrusts.
Abdominal Thrusts
If back blows are ineffective, deliver up to 5 abdominal thrusts.
Performed standing behind the casualty. Place your fist between the casualty’s umbilicus and xiphisternum, grasp this fist with other hand, pull forcefully inwards and upwards.
After each abdominal thrust check if obstruction has cleared.
Abdominal thrusts are contra-indicated in pregnant women and in infants (children under the age of 1 year). Perform chest thrusts instead: in pregnant women, position encircled arms so that hands are at the base of the sternum rather than between the umbilicus and the xiphisternum. In infants, follow the guidance under paediatric considerations below.
Alternate between 5 back blows and 5 abdominal thrusts until obstruction is cleared, or the casualty becomes unconscious.
Consider the early application of high-flow oxygen, if available and resources allow.
Consider applying monitoring, if available and resources allow. SpO2 and EtCO2 monitoring should be applied if initial actions have not immediately cleared the obstruction.
If the airway obstruction is not clearing, prepare to commence CPR when the casualty loses consciousness.
Unconscious casualty with airway obstruction
Commence CPR.
Perform chest compressions, defibrillation and ventilation as normal in accordance with your level of Life Support training (BLS/ILS/ALS).
When assessing and managing the airway, consider the following;
If visible obstruction in oropharynx, attempts to remove this should be made with Magill forceps under direct vision.
A sweep with a single finger to remove a visible airway obstruction can be attempted if Magill forceps are not available. Avoid blind finger sweeps as these might push an obstruction further into the airway.
If Magill forceps are not available then use of suction equipment under direct vision can be considered. Again, caution must be taken to not worsen the situation by forcing any obstruction further in.
If a laryngoscope is available and the practitioner is competent in its use then use laryngoscopy to attempt to visualise obstruction. If visualised, attempt removal with Magill forceps.
If CPR is ongoing, and all attempts have failed to secure an adequate airway to allow ventilation, proceed to emergency cricothyroidotomy. However, an emergency cricothyroidotomy must not interrupt or delay the delivery of basic life support.
Advanced Assessment & Management
The initial assessment and management of a choking casualty will initially follow the same steps described above in a deployed surgical/hospital facility, but with additional resources likely to be available, early consideration should be given to the following:
Request immediate assistance of available airway specialists such as anaesthetist, intensivist, ENT surgeon or maxillofacial surgeon. Airway specialists may consider advanced airway management strategies beyond the scope of this guidance. Advanced airway management should be led by the most experienced airway specialist available at the facility.
Applying high-flow oxygen and ensure available physiological monitoring is attached.
In a patient in cardiac arrest secondary to foreign body airway obstruction:
Repeat airway assessment using laryngoscopy and Magill forceps if a definitive airway has not already been secured.
Do not delay proceeding to establish emergency front of neck access (eFONA) - usually an emergency cricothyroidotomy as per the surgical airway guideline unless specialist skills are available for other procedures.
Prolonged Casualty Care
A patient with severe foreign body airway obstruction is a time-critical emergency. There is little scope for prolonged casualty care as these patients will likely rapidly deteriorate to cardiac arrest secondary to hypoxia. In this event refer to Immediate Action above.
Prolonged resuscitation efforts in a patient in cardiac arrest secondary to foreign body airway obstruction must be considered in the context of the tactical, situational and resource limitations at the time. Where possible, emergency cricothyroidotomy and attempted ventilations with any available oxygen should be considered before stopping resuscitation efforts.
In patients with persistent mild foreign body airway obstruction then early evacuation to facilities equipped with specialist airway and surgical capabilities is essential.
Allow the casualty to assume a position of comfort and encourage them to continue coughing.
If not already commenced, oxygen should be provided to mild FBAO casualties to maintain SpO2 >92%. EtCO2 should be attached if available.
Repeated monitoring of physiological trends should be recorded.
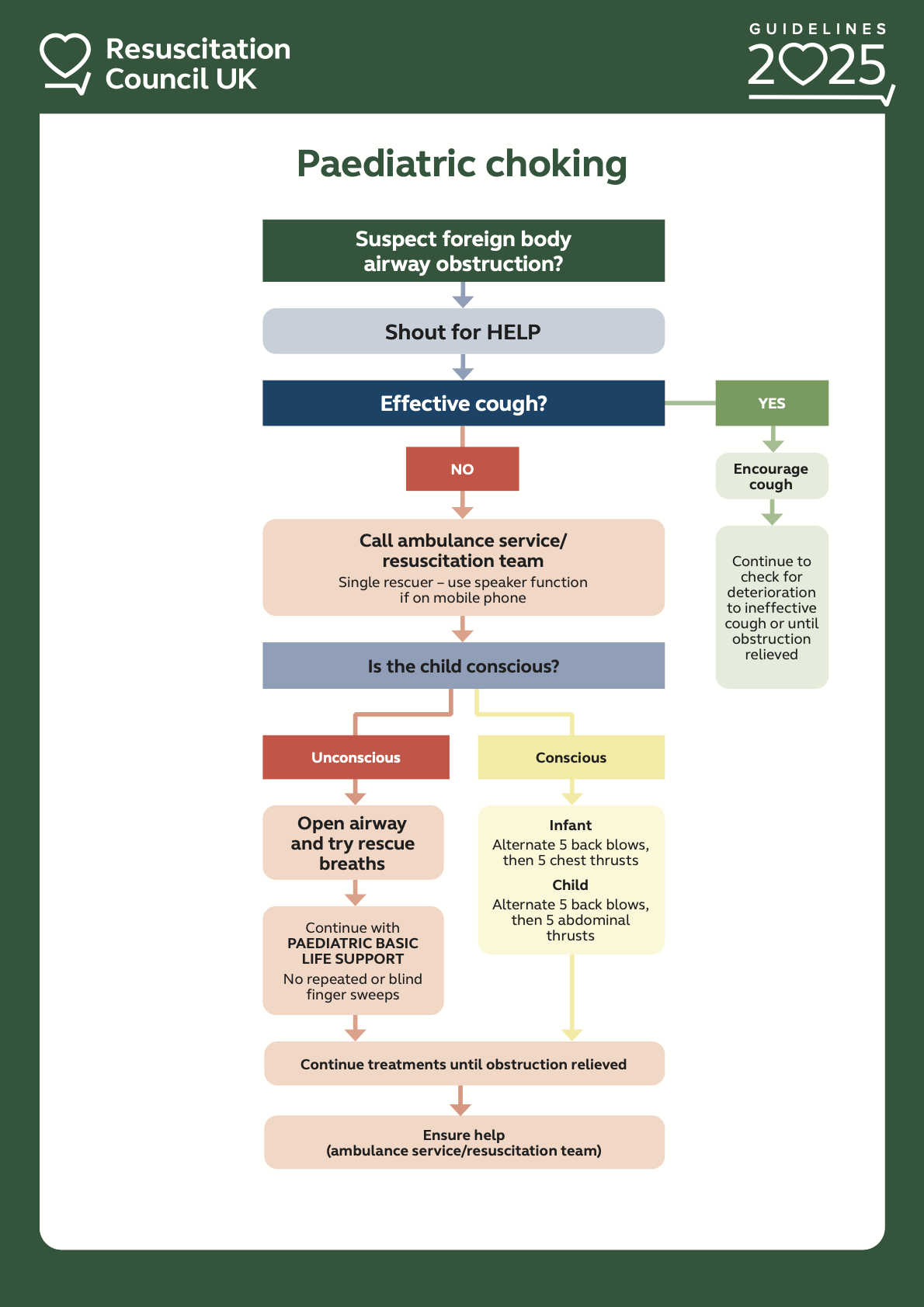
Paediatric Considerations
Immediate actions follow the same principles with specific modifications in smaller children:
In all children presenting with foreign body airway obstruction ensure additional / expert help has been requested if available.
If the child is able to cough, encourage them to do so. If unable to cough, or if cough is ineffective this is severe airway obstruction.
Infants (children under the age of 1 year)
Back Blows
Lay the infant face down on your forearm, support their head with your hand.
Aim to hold their head below level of their chest.
Deliver a forceful blow between their shoulder blades.
Check if obstruction cleared after each blow.
After 5 Back Blows if obstruction remains, proceed to Chest Thrusts.
Chest Thrusts
Lay infant on their back - either on a firm surface or on your knees.
Encircle the infants chest with your hands, place thumbs over their sternum.
Sharply compress the sternum using your thumbs.
Check airway and in mouth to assess if obstruction has cleared after each Chest Thrust.
Continue to alternate between 5 back blows and 5 chest thrusts until obstruction cleared, or child loses consciousness. If the child is, or becomes unconscious start CPR in accordance with paediatric life support algorithms - including attempting to perform 5 rescue breaths before commencing chest compressions.
Children (over the age of 1 year)
Follow immediate actions as for adults above.
If the child is, or becomes unconscious start CPR in accordance with paediatric life support algorithms - including attempting to perform 5 rescue breaths before commencing chest compressions.
Resolved Foreign Body Airway Obstruction
A casualty presenting following a resolved episode of foreign body airway obstruction must be thoroughly assessed and examined.
Potential complications include negative pressure pulmonary oedema and adult respiratory distress syndrome (ARDS). Imaging of the chest is needed if the if casualty has respiratory distress and/or hypoxia that develops or persists after the choking episode resolves.
If there is any suspicion of possible aspiration - including in cases of mild/resolved foreign body airway obstruction - prophylactic antibiotics should be administered in accordance with current DMS antimicrobial guidelines.