SILVER (OUTER) CORDON
• The 'warm' zone that defines the safe boundary within which activity supporting the incident is managed.
SILVER COMMAND POST
• The command and control point for all activity within the Silver cordon.
BRONZE (INNER) CORDON
• Referred to as the ‘hot' zone. It is a high threat environment that requires expert risk assessment.
BRONZE SECTORS
• The Bronze cordon may be divided into sectors to improve control.
BRONZE COMMAND POST
• The incident command and control point for all Bronze Commanders.
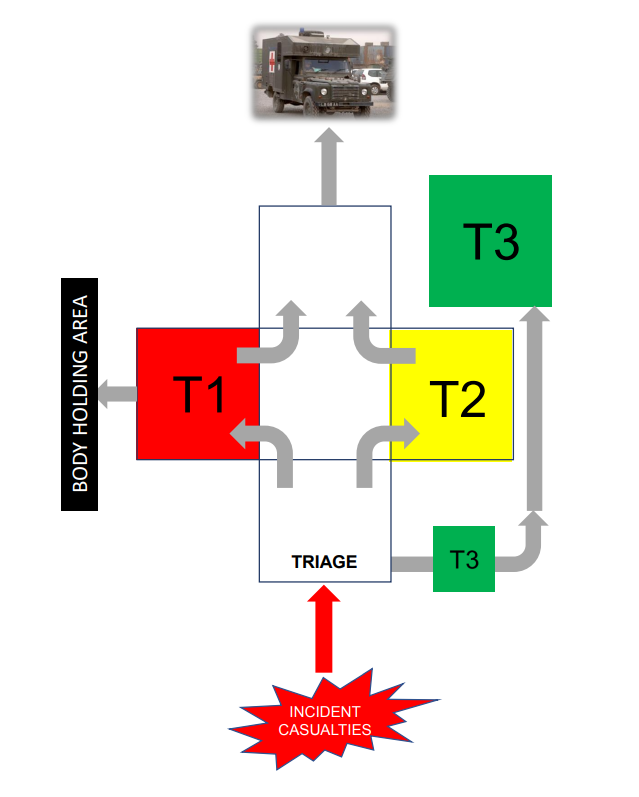
CASUALTY CLEARING STATION
• A temporary medical treatment facility that provides life saving medial treatment prior to evacuation to definitive medical care.
SURVIVOR RECEPTION CENTRE
• A location within the Silver cordon where personnel with no obvious or very minor injuries are managed.
AMBULANCE PARKING POINT
• The location where vehicles required for casualty evacuation are parked.
CASUALTY LOADING POINT
• Located at the rear of the Casualty Clearing Station. Casualties are loaded onto suitable transport for evacuation to definitive medical care.